Projects ECG (Electrocardiogram) Monitoring
R Axis deviation using Phase space
The R axis deviation obtained using the limb lead (lead I, II, III) is used for electrocardiogram diagnosis. In this article, I introduce a method of calculating the R axis deviation from a single lead under mobile ECG measurement conditions such as smartwatches, which have no choice but to use a single lead.
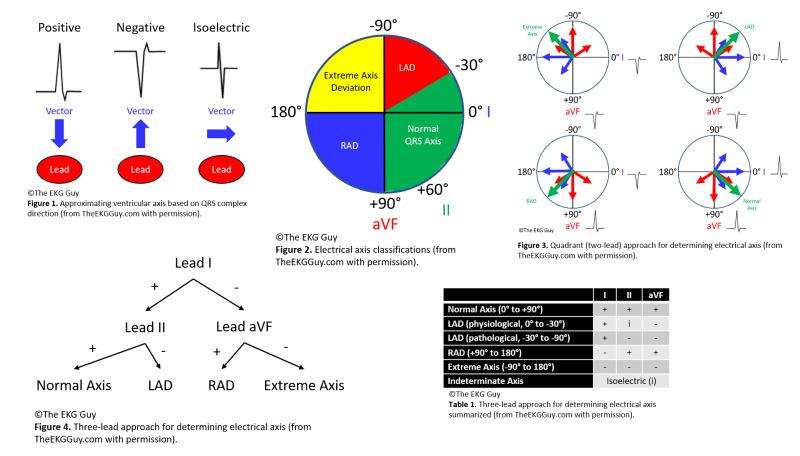
Fig.1 R Axis Deviation
The electrocardiogram signal has no phase information. Therefore, using electrical axis classification of Leads I, II, and III, a rough phase is obtained using several methods, as shown in Figure 1, and is used for diagnosis.

Fig.2 R wave morphology
Five years ago, I obtained the phase of the ECG using the Hilbert transform and attempted to diagnose the ECG based on
the phase information. The attempt using Lead II was showing very encouraging results.
However, under electrocardiogram measurement conditions such as smartwatches, Lead II measurement had the fatal
disadvantage of being very inconvenient.
Lead I had the convenience of measuring ECG by touching the knob of the smartwatch with the right or left finger, but
most of the R waves in the ECG data I was using had the form of qRs in Fig.2.
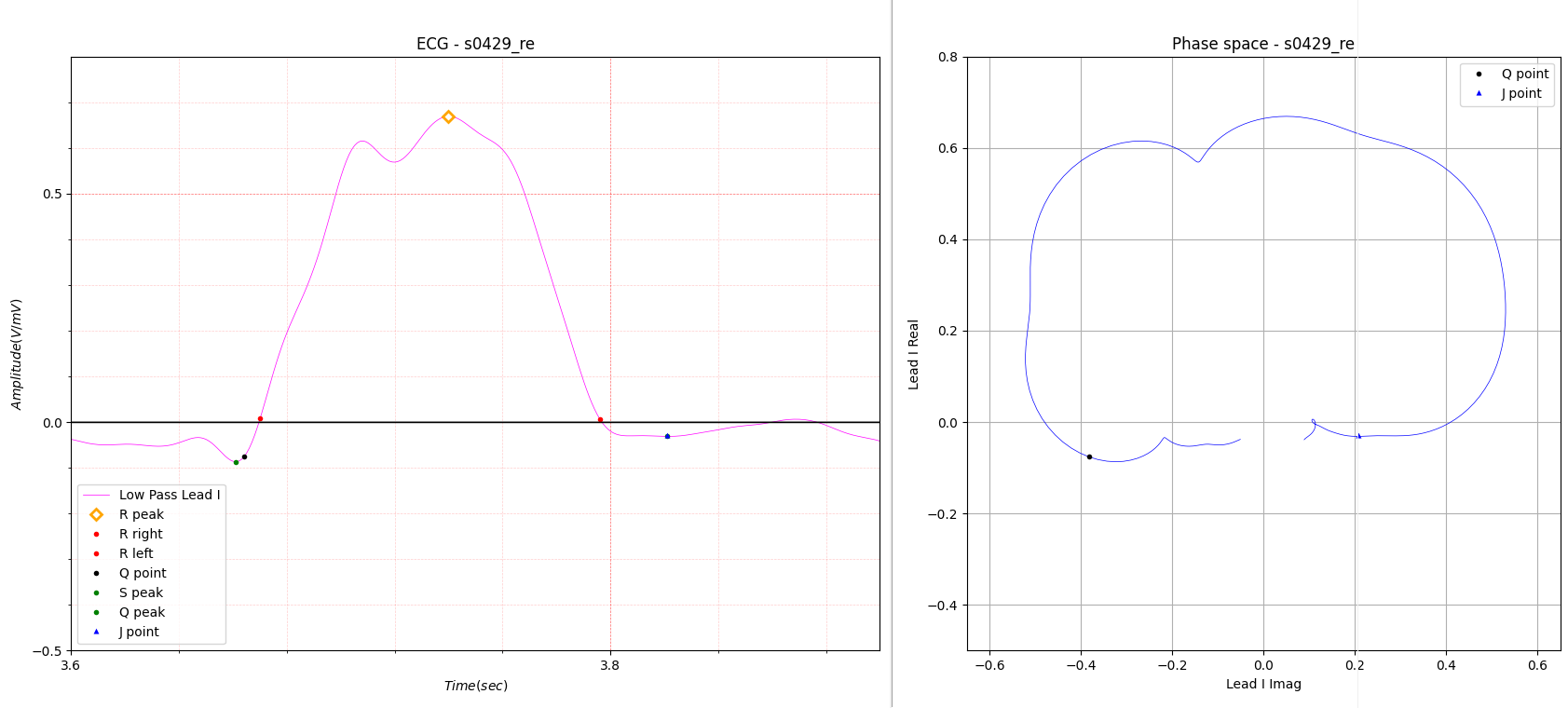
Fig.3 Example of R axis deviation using phase space
Fig. 3 schematically illustrates how to obtain the R axis deviation using phase space of a single lead.
QRS amplitude represents the sum of the vectors of R peak, Q peak, and S peak.
QRS amplitude A is the peak of the imaginary part added to each peak.
Fig. 3 is a special case that is not in the morphology of Figure 2.
This is different from the commonly used QRS amplitudes here.
QRS amplitudes here refer to the vector sum of each peak using phase space.
Most QRS amplitudes in Lead I were close to vertical, so it was thought to be difficult to use for ECG diagnosis. On the
other hand, Lead II shows various forms that are very advantageous for electrocardiographic diagnosis. This is also the
reason why most doctors, when asked to choose one lead when reading an electrocardiogram, choose lead II without
hesitation.
What overcomes the disadvantages of Lead I in electrocardiogram analysis is that even though there is a tendency for QRS
amplitudes to become vertical in Lead I, in case of heart disease symptoms, it appears in the axis deviation of the T
wave and P wave.
The T wave axis deviation will be introduced in the next post.
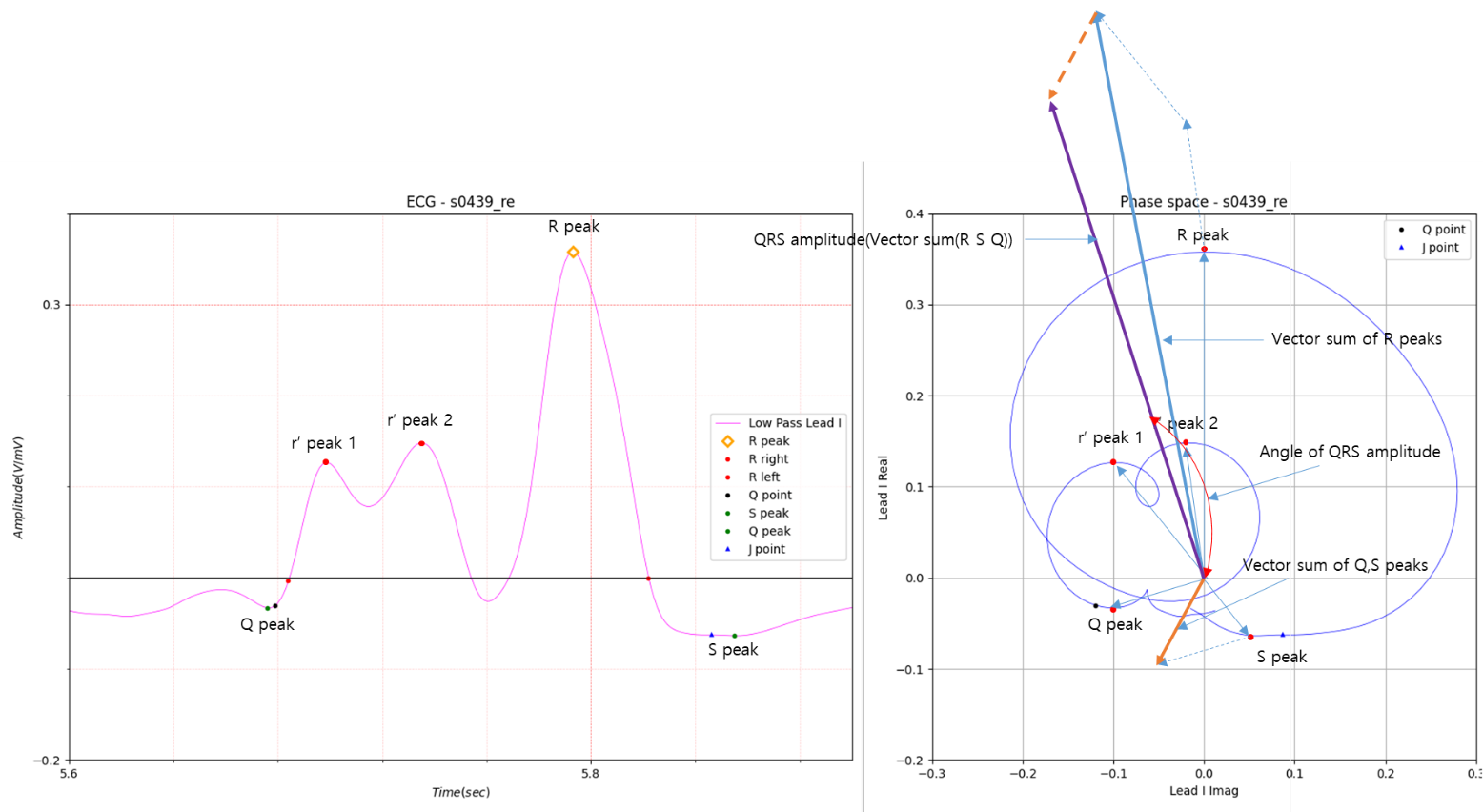
Fig.4 R axis deviation of Multiple R waves
QRS Amplitude:0.603, R axis deviation: -16.658
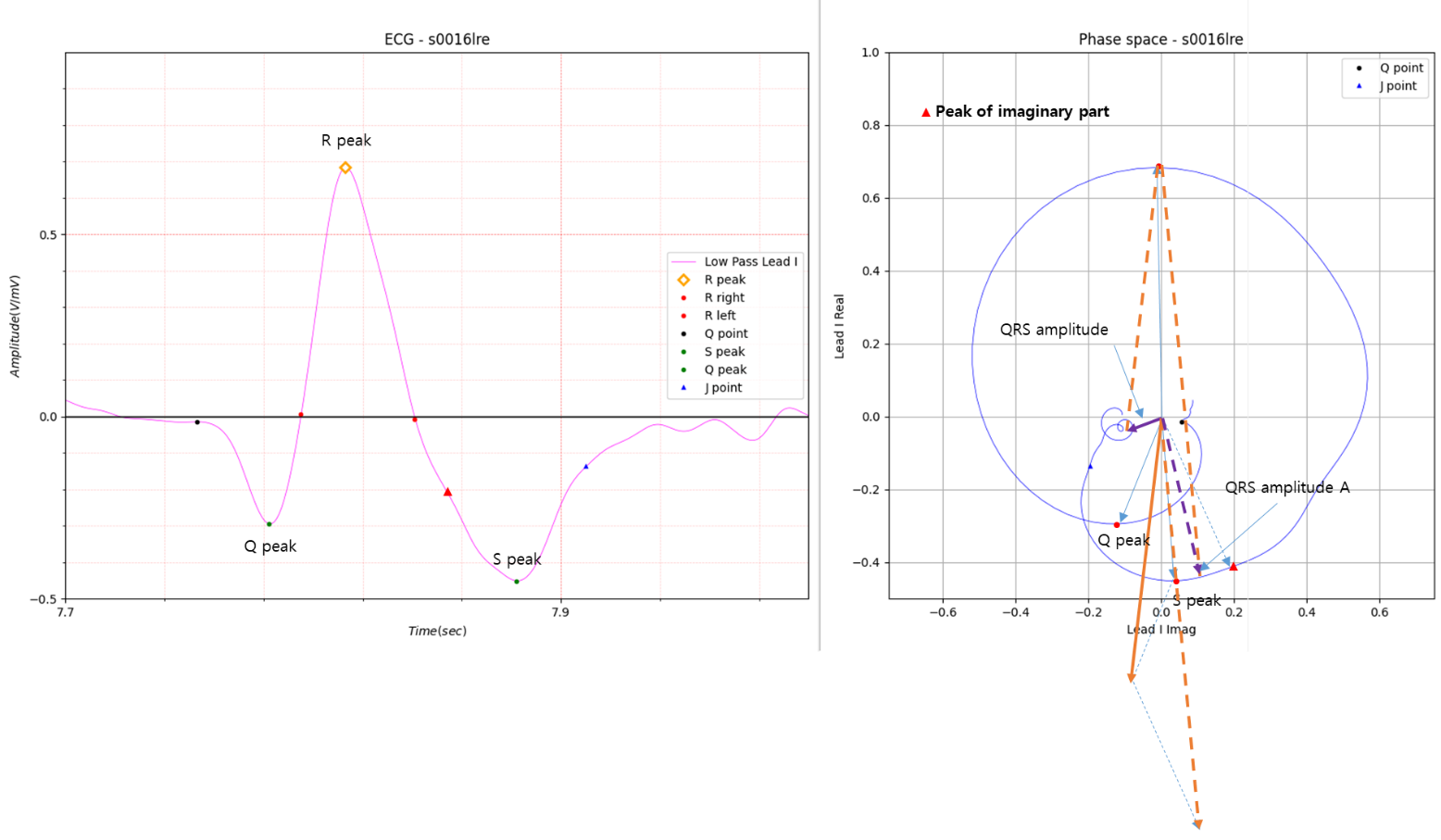
Fig.5 Example of R axis deviation
QRS Amplitude: 0.113, R axis deviation: -123.97
There is a question as to whether T and P morphology, as well as R wave morphology, are actually used for diagnosis. I
have used each morphology for diagnosis, but it was difficult to create software because the program was too complex.
I'm not a very good programmer. In order to make up for the lack of skills, I am naturally seeking an easy path.
Is morphology simply used in textbooks for ECG education?
What could be a very simple alternative to Morphology?
That is the Axis deviation covered in this post.
Two types of Premature Ventricular Contraction (PVC) are shown below.
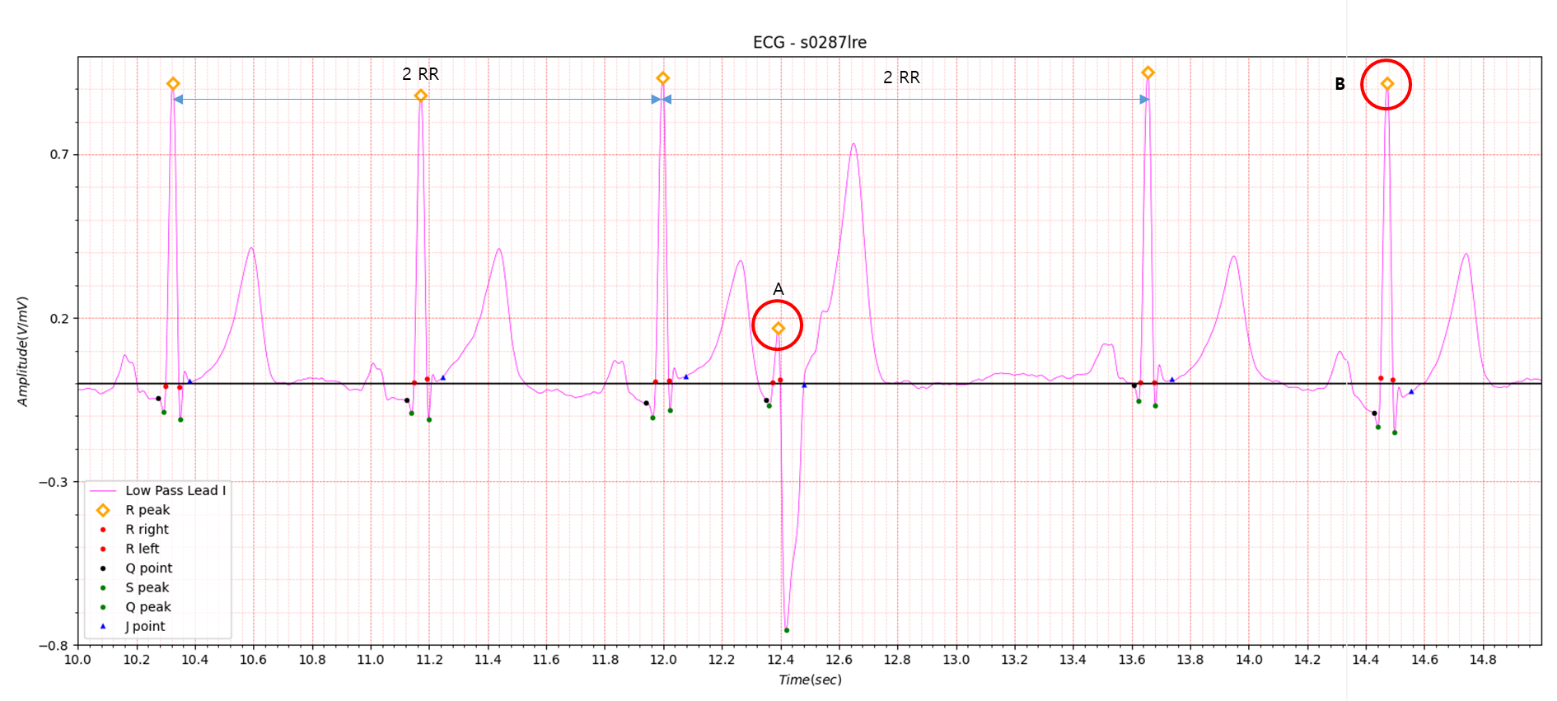
Fig.6 Type A PVC
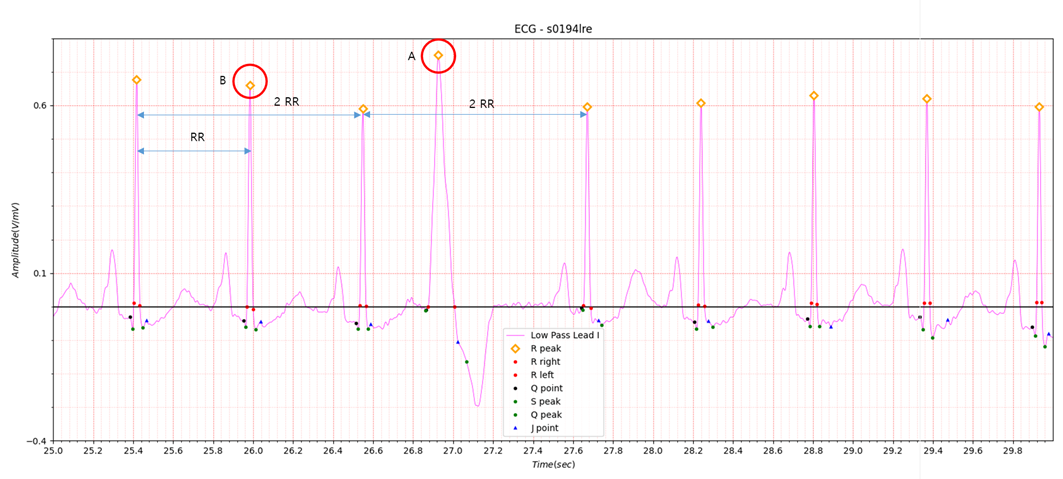
Fig.7 Type B PVC
As for PVC, it is linked above, so the explanation will be omitted. In Fig.6 and Fig.7, the amplitude of part A where
PVC occurs is different. In Fig.6, the amplitude of part A where PVC occurs is lower than that of other R peaks. On the
other hand, in Fig.7, the amplitude of part A where PVC occurs is higher than that of other R peaks.
The presence of these two types interferes with diagnostic work.
The R peak to R peak interval time (heart rate RR) before and after PVC occurrence has a minimum value before PVC
occurrence and a maximum value after PVC occurrence. However, this trend is observed in some cases where arrhythmia
occurs even if PVC does not occur. Another peculiarity is that when PVC occurs, there is no T wave.
As you list these features, the complexity of the code increases.
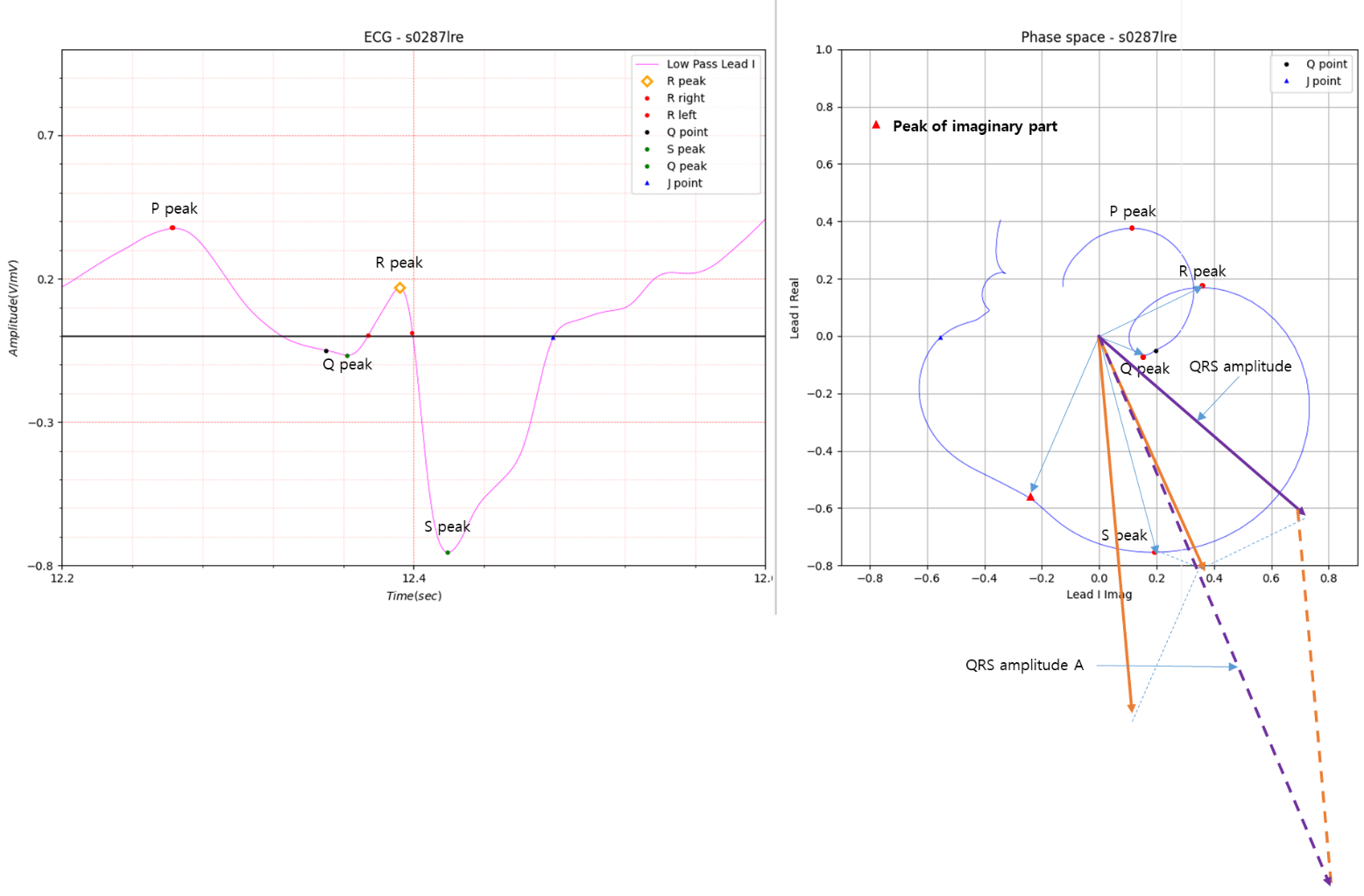
Fig.8 Part A of Fig. 6
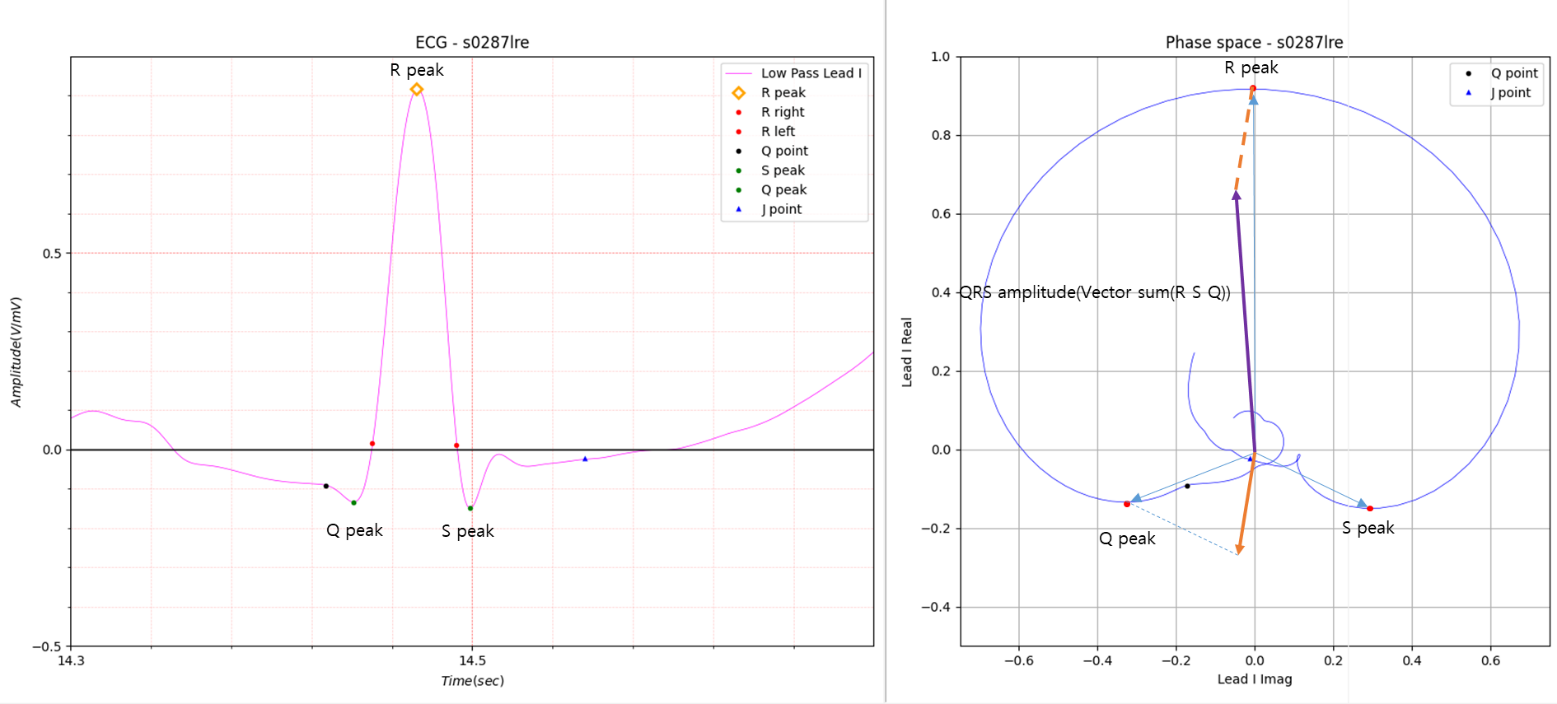
Fig.9 Part B of Fig. 6
Fig. 8 shows the R axis deviation for the occurrence of type A PVC in Figure 6.
The results are as follows:
QRS Amplitude: 1.056, R axis deviation: 128.67
Fig. 9 shows the R axis deviation in the steady state.
The results are as follows:
QRS Amplitude: 0.620 R axis deviation: 1.44
Statistics for all R axis deviations are as follows:
R axis deviation Amplitude: Number of R: 35, Avg: 0.796, Max: 1.056, Min: 0.62, std: 0.088
R axis deviation Angle: Avg: 7.8, Max: 135.449, Min: -8.99, std: 30.981
A total of 35 R axis deviation results are shown below.
35 [1.073 10.916 4.874 3.931 2.313 -7.416 1.758 -2.265 1.1428 -2.768 -2.029 -8.990 2.258 128.671 7.830 1.435 2.661 0.193
-8.630 10.17 135.449 10.479 -5.413 -1.496 -0.24 1.066 1.173 0.254 -0.338 -3.877 -1.334 -0.662 2.788 -4.626 -7.362]
The area highlighted in red is the area where PVC occurred. I don't think this method is the best. Because someone may
be diagnosing it in a better way. However, when PVC occurs in a single lead, finding the R peak itself can be difficult.
Even if R peak cannot be found, there is no major difficulty in diagnosing arrhythmia. This is because if you miss the
peak, the RR of that part will be twice as high as the RR of other parts. It goes without saying that eliminating these
errors increases the reliability of diagnostic software.
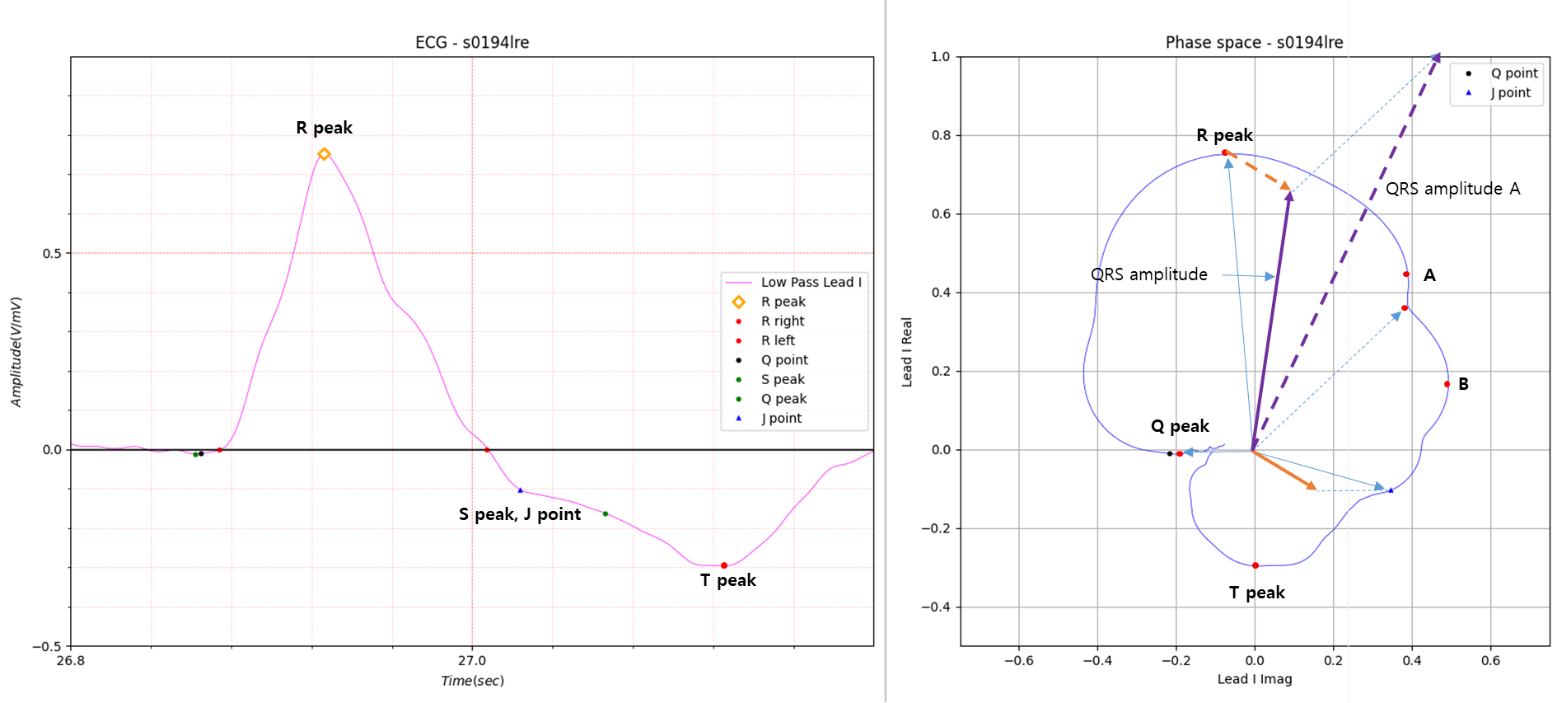
Fig.10 Part A of Fig.7
Fig.10 is the part where PVC occurred in Fig.7.
The figure shows two methods: QRS amplitude and QRS amplitudeA.
The QRS amplitudeA vector was obtained by including the notch part, not the peak.
In the figure above, A and B indicate the peak of the imaginary axis. The notch between peaks A and B is the imaginary
part peak.
The results in Fig.10 are as follows.
QRS Amplitude: 1.024, R axis deviation: 21.56
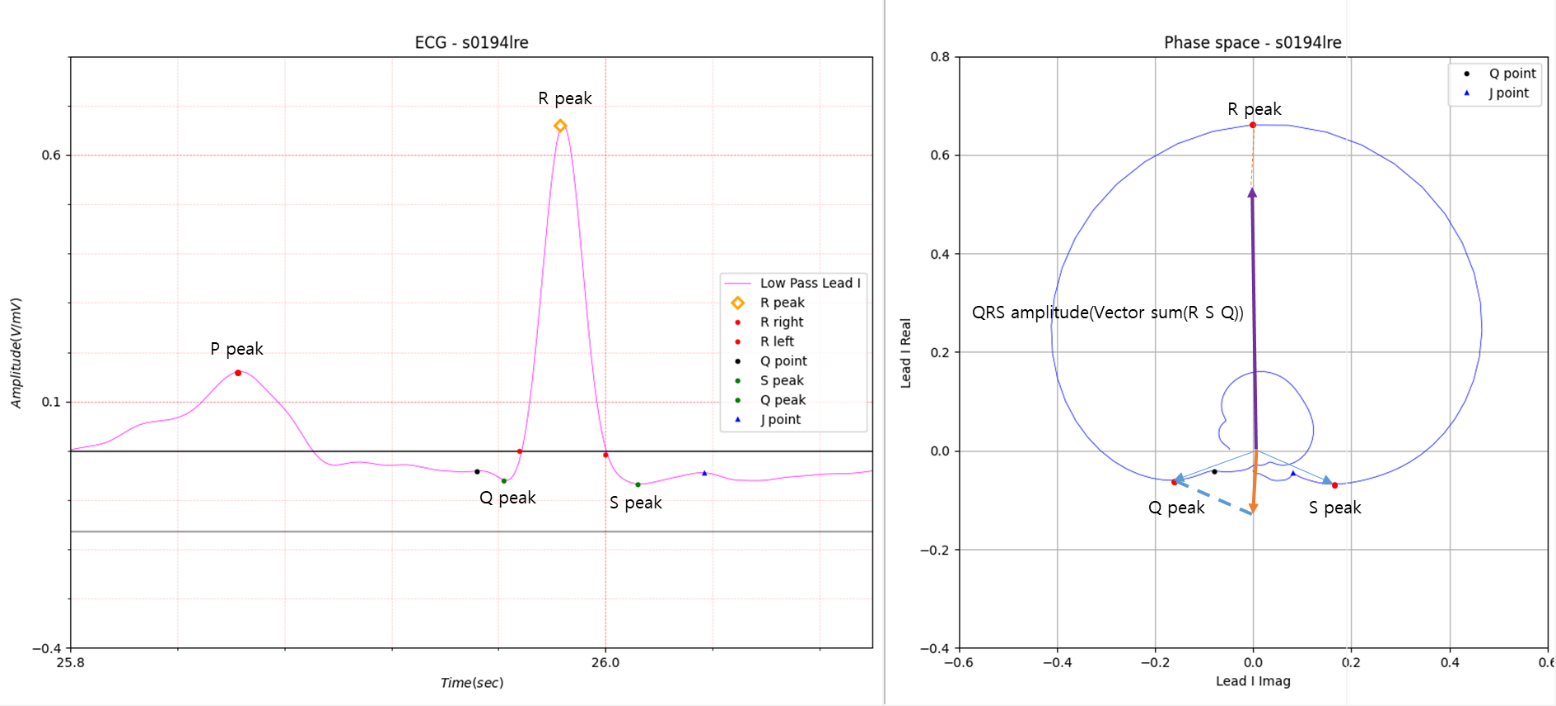
Fig.11 Part B of Fig. 7
Fig.11 schematizes the R axis deviation of the steady state in Fig. 7.
The results are as follows:
QRS Amplitude: 0.533, R axis deviation: -0.20
The R axis deviation statistics of Data s0194lre are as follows.
R axis deviation Amplitude: Number of R: 55, Avg: 0.523, Max: 1.123, Min: 0.391, std: 0.109
R axis deviation Angle: Avg: 1.795, Max 25.779, Min -10.306, std: 7.218
The above results seem unsuitable for diagnosing PVC of the type (tall and thick) shown in Fig. 7.
In this case, you can use the R peak width introduced in the previous post.
R peaks width:
55 [ 29 31 33 36 37 38 39 32 29 28 29 32 35 37 42 35 39 31 30 29 29 31 32 37 40 35 36 37 31 30 29 30 31 33 38 37 37 37
40 36 32 30 29 31 32 32 133 36 33 31 29 27 124 30 33]
The data introduced in Figure 3 is not shown in the morphology introduced in Figure 2, but can be viewed as type rr'.
This is something that needs to be considered in the future.
This post ends by introducing the basic concept of R axis deviation and simple use cases.